Chronic venous insufficiency (CVI) is a common condition that is typically accompanied by lower limb oedema, trophic skin changes and discomfort, secondary to venous hypertension.
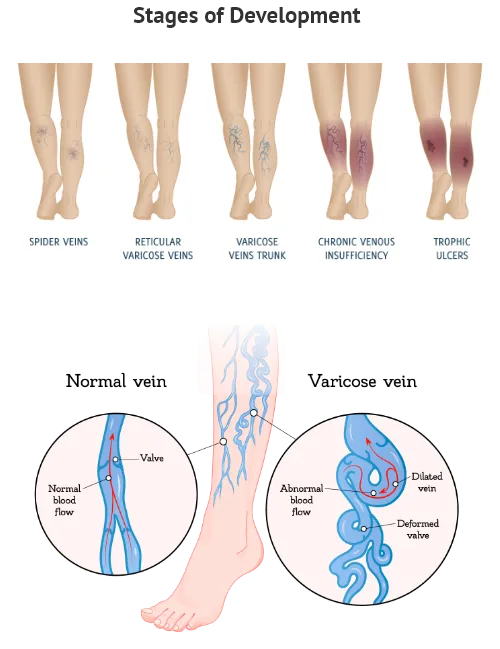
Our veins are responsible for the return of blood back to the heart. It is a one-way system, controlled by valves at every 0.5-1cm increments.
CVI, is the result of damaged or dysfunctional valves, within which the pressure gradually increases, further damaging their endothelium walls, allowing leakage of fluid, proteins cellular material and blood into the tissues.
Causes of Chronic Venous Insufficiency (CVI) include:

- reflux due to valve incompetence due to malformations or congenital absence of valves
- obesity (hydrostatic pressure)
- pregnancy (hydrostatic pressure)
- prolonged standing or dependent immobility (gravity associated hydrostatic pressure)

- ageing
- calf muscle pump failure
- deep venous thrombosis/obstruction (DVT)
- luminal fibrosis (due to cellulitis, surgery, or trauma)
CVI leads to venous stasis, venous hypertension and increased filtration into the interstitial tissues resulting in oedema.

As the blood capillary pressure rises, red blood cells are also forced out into the tissues. As they break down, they leave behind iron bound to protein (haemosiderin) which causes a brown staining of the skin.

Other symptoms of CVI include thickening of the skin and tissue fibrosis. In advanced cases, individuals may develop lipodermatosclerosis, which gives a ‘woody’ appearance and texture to the leg.
Classifications of Chronic Venous Insufficiency
- Reversible oedema, dark blue skin discolouration at the medial and lateral edge of the foot.
- Irreversible oedema: hemosiderin deposit, dermatosclerosis, varicose eczema, cyanotic skin colour, severe tissue tension, and phleboedema
- Ulcus cruris (ulcers)
- Positive family history, age, and lack of exercise are considered risk factors.
What are the early signs of CVI?
What are the early signs of Chronic Venous Insufficiency?
Spider & Varicose Veins ~ Spider Veins are small damaged blood vessels. Can be caused by either sitting or standing for long periods constantly, adults of a mature age, pregnancy can be a cause or due to injury.
Varicose veins are a clear indication of damaged valves within the blood capillaries and are a clear sign of venous insufficiency.
Skin Discolouration Blue/Brown ~ The bluish skin could be a sign of an arterial flow problem, and needs further investigations with your vascular specialist or podiatrist. The brownish discolouration is that of iron rich blood that has settled into the tissues (hemosiderin staining)
Some common conditions associated with hemosiderin staining include:
- trauma
- leg oedema
- diabetes
- cardiovascular disease
- high blood pressure
- venous ulcers
- venous hypertension
- vein insufficiency
Swelling ~ dynamic oedema particularly at the end of the day. Reversible by elevating your legs in early stages. If irreversible it is developing into more severe stages.
Ulcers ~ This is in fact more towards the later stages, but an identifiable reason for treatment urgently. However, treatment differs to the type of ulcer/s. Venous ulcer compression is ok, Arterial Ulcer is a definite NO for compression, until it has been investigated for severity.
What is Phleboedema?
What is Phleboedema?
Long term overload of the lymphatic pathways is considered the cause of phleboedema. Particularly during the second half of the day, the patient suffers stasis and swelling in the legs. Once the tissue is chronically indurated, the lymph vessels are damaged.
A positive stemmer sign confirms lymph drainage disorder that leads to oedema. Therefore diagnosed as Phleboedema.
Stages of CVI turned Phleboedema
Stages of Chronic Venous Insufficiency (turned) Phleboedema
Stage 0 – Latent
- No symptoms
- No visible/palpable oedema
- Lymph-vascular compensation of ambulatory venous hypertension.
Stage 1
- Overnight reversible perimalleolar oedema (mild)
- Corona phlebectatica (ankle flare)
- Dynamic insufficiency of the lymphatic system
- Reduces with elevation
- Low-protein oedema
- Upon waking in the morning the limb or affected area is almost a normal size.
- Mild pitting in lower leg / ankle
Stage 2
- Persistent oedema up the middle of the lower leg
- Hyperpigmentation (purple/browning colour)
- Safety valve insufficiency of the lymphatic system
- Irreversible oedema (moderate)
- Accumulation of protein rich edema fluid
- Deep pitting oedema mostly in lower leg / ankle
- Varicosis
- Hemosiderin deposits
- Sensation of heaviness / tension / leg cramps
- Elevation of leg relieves condition
Stage 3
- Ulceration
- Compartment Syndrome
- Drop Foot
- Fibrosis and sclerosis (severe induration)
- Skin changes
- The tissue at this stage is hard (fibrotic) and will only be slightly responsive to the touch.
Complications
- Thrombosis
- Embolism
- Ulceration
- Phlebitis
- Phlebolymphoedema
Treatment for CVI / Phleboedema
Treatment for Chronic Venous Insufficiency / Phleboedema
The introduction of endovenous modalities reduce the risks, but overall expenses for invasive treatments are rising, and patients are still not offered effective therapy until they show serious problems or at least large varices.
Current efforts are on safety and patient comfort of endovenous methods, like with the second and third generation of vein gluing, the combination of sclerotherapy and compression film bandage, perivenous hyaluronan or novel protein-enforced microfoam. While it is good to improve ablation techniques, it may be much better to reduce the need for it, starting with the early stages. (Innovation in Phlebology / The Future of Phlebology, Johann Christof Ragg, Venous Interventions I, Main Ballroom, May 5, 2019).
Early Intervention
This is where Sal comes in!!
Ultimately, treatment for all venous hypertension requires a detailed study of what may be occurring beneath in your tissues, reasons why it has occurred and treating the cause not just the symptoms.
The gold standard of treatment is compression to assist your venous and lymphatic return. But there are a few things to consider before compression can be prescribed.
- Good Arterial Flow to the extremities
- Neuropathy – Sensation or loss of feeling
- Infection
- Diabetes (Type 2)
- Oedema and reasons for
- Thrombosis
- Other co-morbidities
Sal’s treatment may include:
- Manual Lymph Drainage (if acute thrombosis must wait 4-6 weeks)
- Compression
- Bandaging in oedema reduction phase
- Circular knit garment in maintenance phase
- Elevation of limb
- Calf muscle pump exercises
- Surgery for varicose veins (in extreme cases, where other methods have not worked)
- Treatment of eczema and ulcers (wound management)
If left untreated , it can cause painful swelling, ulcers and open sores, which can lead to infection, or progress to a life-long painful condition called Post Thrombosis Syndrome with continued high risk of other thrombosis.
Other Treatment options available in clinic with Sal
- (MLD) Manual hands-on lymphatic Drainage
- Combined (MLD) & Pneumatic Compression Pump
- Pneumatic Compression Pump only sessions (45mins)
- Decongestive Therapy – Bandaging & Garment prescription
- Wound/Ulcer Management
- Scar & fibrosis management
- Low Level Laser Therapy
- Muscle & Myotherapy treatments (see muscle pages for details)
Garment Recommendations
More information to be added at a later date. In the meantime, for garment information and to ensure you are measured correctly, head to the top of the page to jump in online bookings, book an online consult or if you are local book a face to face for more info.
