What is Oedema?
Oedema is an accumulation of fluid, awaiting removal and backing up due to a slow or overworked lymphatic system (LS) or has been left stagnant in the connective tissues due to damaged or malformation of the lymph vessels.
There are a number of reasons why we may be affected by oedema.
It can be due to some major health concerns (see my list further below) or for otherwise healthy and general swelling, it can depend on heat (the weather), lack of movement (immobility), being on your feet all day (mostly standing), nutrition inbalance (lack of quality protein intake), pregnancy, or for the purpose of what Sal does, a damaged lymphatic system.
Here is a quick reference on what to research (under Conditions tab) if you have:
- Swollen lower legs & feet – bilateral (Venous Insufficiency page)
- One limb (arm or leg) larger than the other (Lymphoedema page)
- Excess fat areas (unaffected by diet and exercise), heavy painful legs or arms, lumpy / bumpy legs or arms (Lipoedema page)
- Swelling after cancer treatment (Cancer Care & Lymphoedema page)
- Swelling after cosmetic Surgery (Surgery Care page, under the Lymphatics header)
To explain why we experience oedema, it may be easier to start with the function of the lymphatics, or in the case of oedema, the dysfunction of the lymphatic system.
The lymphatic system (LS) is in charge of moving the oedema out, and
In a good working lymphatic system, without injury or cause for slowing down, it operates at around 20% of it’s capacity. Therefore allowing 80% in reserve in case of an event/injury.
Now, if we add injury, inflammation, surgeries, hormone changes, ageing, less activity, poor diet to the mix, just to name a few… will definitely impact the smooth running of the lymphatics, giving it more debris, disease and other inflammation to deal with and remove.
I hope this is making sense and you are still following………..
In the short term, our lymphatic system can usually recover quickly, as it still has plenty of space and capacity in reserve. But if this occurs too frequently, or over a long period of time, it has the potential to slow down the system (impeding repair), creating a lot of backfill that compounds what I’ve described above 10 fold, due to constant stress and wear and tear on the lymph vessels.
It then becomes a roll-on effect, slowly decreasing capacity as the vessel walls become compromised, and progressing into lymphatic dysfunction and lymphatic conditions.
Here are some of the other causes for oedema that will have an impact on the overall lymphatic system as described above:
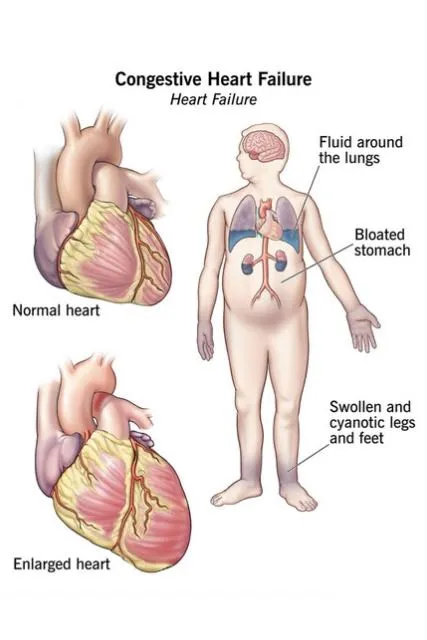
- Heart conditions: Such as heart failure or cardiomyopathy
- Kidney disease: Can cause oedema
- Liver disease: Such as cirrhosis
- Lung disease: Chronic lung disease can cause oedema
- Thyroid disease: An underactive thyroid can cause oedema
- Malnutrition: Not having enough of the right foods can cause oedema e.g. inflammatory foods, poor quality or insufficient protein
- Medications: Some medications, such as some antibiotics, corticosteroids or high blood pressure (hypertension) medicine, can cause oedema
- Pregnancy: Oedema related to pregnancy, short term unless complicated by other co-morbidities
- Menstrual cycles: Oedema related to menstrual cycles can be treated with manual lymph drainage. Sal has had great success with this
- Injuries: Such as a strain or sprain
- Insect bites or stings: An insect bite or sting can cause oedema
- Allergic reactions: A large allergic reaction can cause oedema
- Head injuries: A blow to the head can result in an accumulation of fluid in the brain
- Strokes: A major stroke can result in brain swelling
- Brain tumors: A brain tumor will accumulate water around itself
- Venous Insufficiency: Increase in blood pressure in the vessel, increases permeability on the walls, resulting in increased water filtration into the tissues
- Lymphoedema: resulting due to damaged lymphatic vessels and chronic oedema
Chronic Oedema
Chronic oedema is defined as oedema of a body part lasting more than 3 months, irrespective of the cause.
This cause may include for example, immobility, venous insufficiency, heart failure, obesity and/or lymphoedema, but each individual presentation is often complex with multiple components at play.
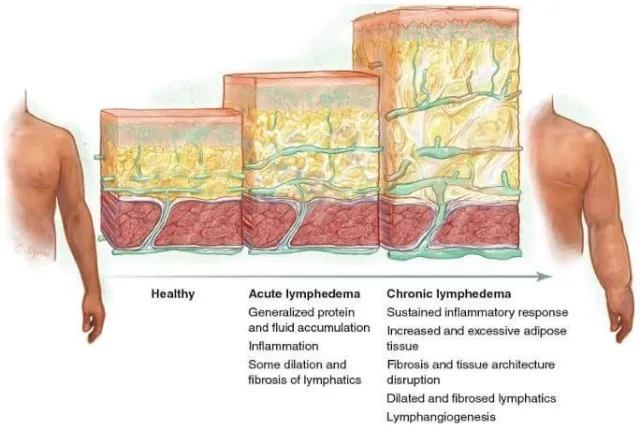
Although the pathophysiology of chronic oedema and lymphoedema may differ, the terms are today often used interchangeably, as the clinical manifestations are often similar (Keast et al, 2015; Mo‑ att et al, 2019b).
Recent research has also shown that there is no net absorption of tissue fluid by the capillary bed, as previously thought, and that all tissue fluid is mobilised by the lymphatics (Mortimer and Levick, 2004). Therefore, it has been argued by some that all chronic oedema can be regarded as an overload of the lymphatics and thereby lymphoedema (Mo‑ att et al, 2019b).
